10+ year ER/ICU RN here.
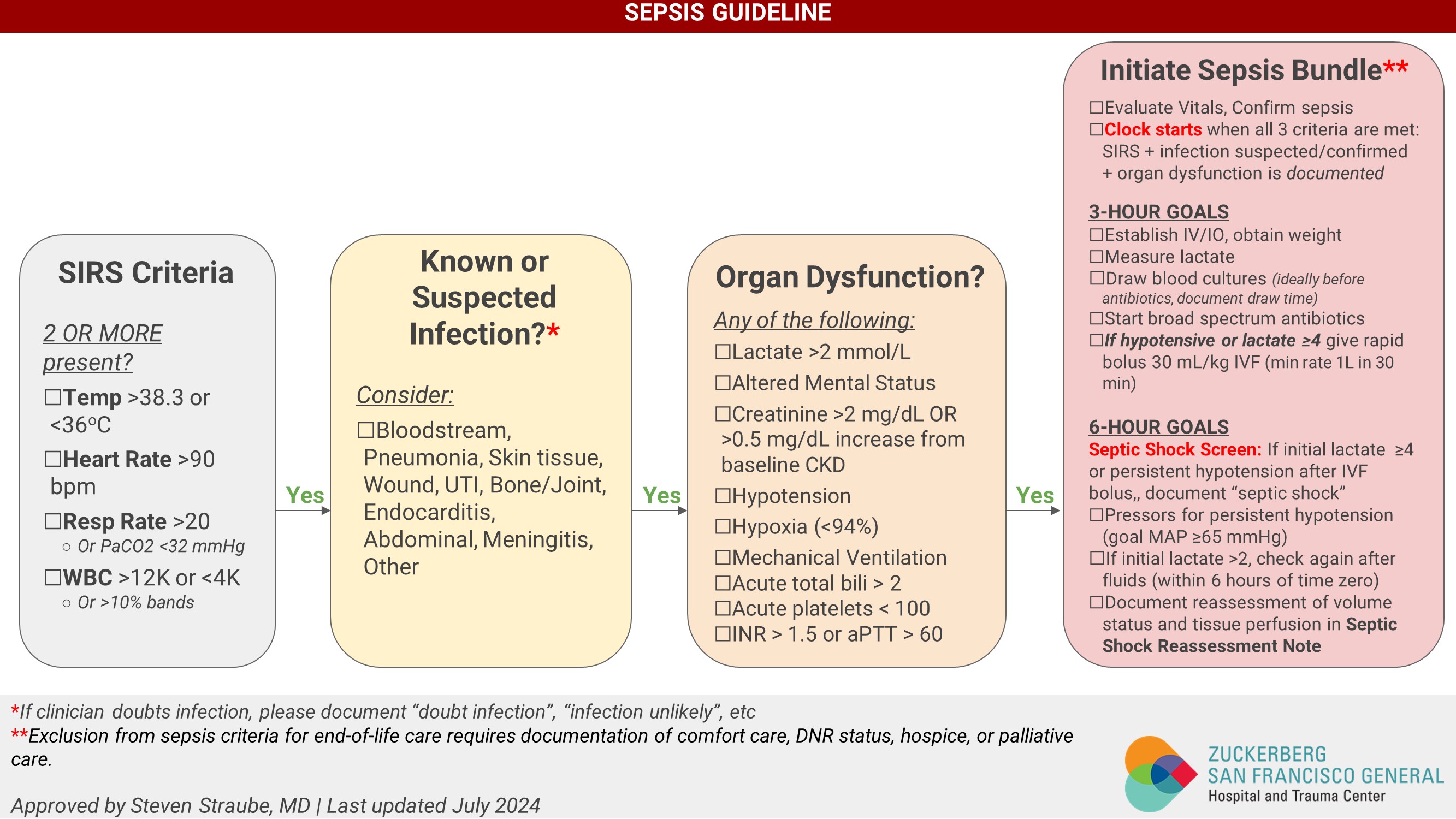
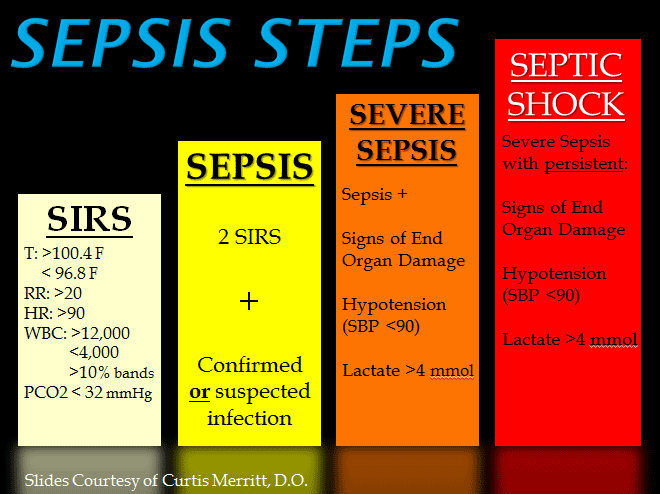
The term "qualifies for sepsis" means next to nothing. It means you had a high heart rate and a fever (typical presentation), which is normal for everything from a low grade fever from a cold, strep, to monkey pox. PS the HR just needs to be above 90.
In terms of the bleeding and what not, an OB asking for an ultrasound in that scenario would be gold standard. Of course you need an US to rule out/in fetal demise as well as know what else may be going on. You do not need an ultrasound specifically for a fetal demise, but, if you suspect one, you want a clear picture. You can just do fetal heart tones on mom which is a bedside task for a nurse that takes 2 minutes. The physician can also do a bedside ultrasound. The physician can also order an US by an US tech that takes maybe 20-30 minutes and can be done in the room at bedside in emergent situations.
In terms of the low blood pressure, that could be from septic shock, or because she was bleeding. I would guess the latter based on available information. Two problems can occur at once, of course.
Pregnant patients that present to emergency departments > 16 weeks, in some places greater than 20, are cleared by E.D. if it is a non-OB related complaint, then evaluated by labor and delivery before discharge. Sometimes they are cleared in ED and sent to L&D for OB related complaints such as lower back pain, abd pain, vaginal bleeding, etc.
There's a lot of layman and litigation talk in these articles covering it. Not something you can rely on in context to an expiration in the emergency department. L&D patients are highly litigious, so suing parties usually get a head start on the release of information.
In addition to that, three ER visits could be an ER problem or it could be a patient problem. I've often had patients that come in for a sore throat like an asshole and come back 3 hours later with chest pain and whoops they have a pulmonary embolism or myocardial infarction, etc. -- there's a reason ER's discharge people with strict return precautions. Even if they weren't going to go in and therapeutically abort a soon to be demise for a septic mother, she would still be admitted on sepsis protocol (which she wasn't because she didn't meet the criteria)...or, for vaginal bleeding, she would be admitted for obs due to the bleeding up to and including transfusions and serial H&H labs. Those first two visits did not present the same as the 3rd. Period.
This poppycock about not addressing medical concerns because of the law are largely hogwash from the articles I've read about this case. People like this receive blood transfusions and sepsis therapy all the time and there is plenty of time to get an ultrasound in the midst of that, which again, would be absolute gold/platinum standard care to do in any state, legal abortions or not. There's a lot of missing puzzle pieces here that will only be found out through courts with a complete and comprehensive review of the medical record as to why the first two visits went the way they did.
They're out in front of their skis with this story as it currently stands, probably due to the election timing.

www.aspirefertility.com
/static.texastribune.org/media/files/b0aeffd550ccb51af53da0ec7dd55771/IVF%20Treatment%20REUTERS%2002.JPG)
 www.texastribune.org
www.texastribune.org